

IBS is diagnosed from your symptom pattern using the Rome IV criteria – a clinical checklist focused on how long you've had symptoms, how often they occur, and how they relate to your bowel movements. It's a positive diagnosis, meaning your doctor is looking for specific patterns that confirm IBS – not just ticking off everything it isn't.¹
If you've spent months, or potentially years, bouncing between appointments, tests, and dead ends, you're not alone. More than a quarter of people wait over five years from their first symptoms to a clear IBS diagnosis² – often because the path isn't explained, the criteria aren't well known, and the pattern of symptoms that defines IBS gets lost in the back-and-forth of ruling things out.
Understanding how IBS is actually diagnosed changes that. It helps you recognize when your doctor has enough to make the call, what tests are genuinely useful versus unnecessary, and when something in your symptom picture warrants a deeper look.
This guide walks through the Rome IV criteria, which tests matter and why, the red flags that change the picture, and what happens once you finally have an answer.
How doctors diagnose IBS: What is the Rome IV criteria?
Under Rome IV, your doctor is looking for recurrent abdominal pain, on average at least one day per week over the last three months, that lines up with at least two of the following:¹
- Pain that gets better or worse when you go to the bathroom
- A change in how often you're going (more or less frequently than usual)
- A change in what your stool looks like (harder, looser, or more variable)
Symptoms need to have started at least six months ago and be ongoing now.
That three-month window is the three-month rule – the minimum pattern your doctor needs to see before confirming a diagnosis.
How the Rome IV criteria protect you from misdiagnosis
These aren't arbitrary boxes to tick. Each one exists to separate IBS from the many other things that can cause gut symptoms – a stomach bug, a food intolerance, a stressful few weeks. If your pain is tied to your bowel habits and it's been showing up consistently for months, that pattern is meaningful. It's what tells your doctor this isn't a passing problem – it's a gut-brain disorder with a recognizable signature.
Knowing the criteria also means you can walk into your appointment ready. If you've been tracking symptoms for three months, can describe how pain relates to bowel movements, and have noticed changes in frequency or stool appearance, you've already given your doctor almost everything they need.
IBS subtypes: why your doctor will classify your IBS
Once IBS is diagnosed and confirmed, your doctor will classify it into one of four subtypes based on what your stool looks like on symptom days. The subtype isn't just a label – it shapes which treatments, medications, and dietary strategies are likely to work for you.¹

How your doctor decides your subtype
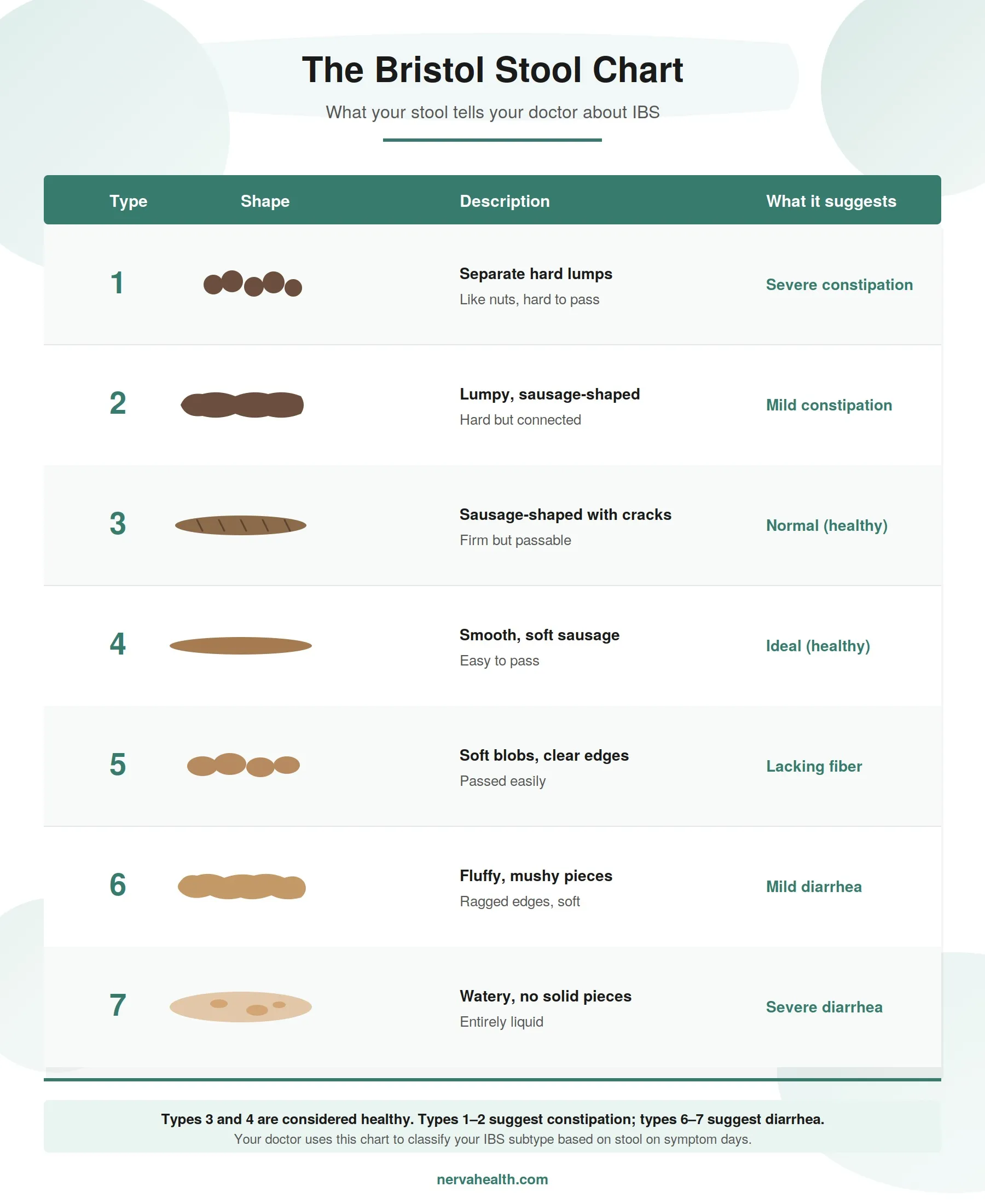
Your doctor classifies your IBS subtype using the Bristol Stool Chart – a visual scale that rates stool consistency from Type 1 (hard, separate lumps) to Type 7 (entirely liquid). Subtype is determined by what your stool looks like on the days you have symptoms, not your "normal" days.¹
This is why tracking matters. Two weeks of stool observations – even informally, with a note on your phone – give your doctor a clear picture of your pattern. Without it, subtype classification often gets pushed to a follow-up appointment.
"The Bristol Stool Chart helps doctors and patients speak apples to apples as far as what is a constipated stool, so type one or two and hard and lumpy and bumpy, or a more loose stool like types 6 and 7, which is more in the diarrhea category. It really helps doctors and patients speak the same language and help you avoid a lot of diagnoses and treatment missteps, because something like constipation can be in the eye of the beholder." – Dr. Justin Brandler, neurogastroenterologist and motility specialist, Virginia Mason Franciscan Health
Why your IBS subtype shapes your treatment plan
Different subtypes respond to different strategies. Some examples:
- IBS-C may benefit from soluble fiber, osmotic laxatives, or medications that increase bowel movement frequency
- IBS-D often improves with loperamide, bile acid binders, or targeted dietary changes
- IBS-M requires a more flexible approach that adapts to shifting symptoms
- All subtypes benefit from gut-brain therapies, which target the underlying visceral hypersensitivity shared across every subtype
That last point is important: while medications and diets are subtype-specific, the underlying gut-brain dysregulation is not. This is why gut-brain therapy is recommended across all IBS subtypes by major guidelines.3
Is there a single test that confirms IBS?
There is no single blood test, scan, or scope that confirms IBS. IBS is a gut-brain disorder – meaning the gut looks structurally normal but behaves abnormally – which is why imaging and biopsies can't detect it. Diagnosis relies on matching your symptom pattern to the Rome IV criteria, supported by a small number of targeted tests to rule out conditions that cause similar symptoms.³
This surprises a lot of people. After months of bloating, pain, or unpredictable bowel habits, it's natural to expect a definitive test that names what's wrong. But the absence of a confirmatory test isn't a gap in medicine – it reflects what IBS actually is. The symptoms come from how the gut and brain communicate, not from tissue damage you can see on a scan.
What about the newer IBS blood tests (IBSchek and IBS-Smart)?
A newer category of blood tests – including IBSchek and IBS-Smart – measures antibodies (anti-CdtB and anti-vinculin) that may be elevated in people who developed IBS after a gut infection. These tests can support a diagnosis of IBS-D or IBS-M, but they have two important limitations:⁴
- They don't detect every case of IBS – a negative result doesn't rule it out
- They're not recommended as a routine diagnostic tool by major guidelines including the American College of Gastroenterology (ACG)
Most gastroenterologists still rely on the Rome IV criteria as the primary diagnostic method, using blood tests as one supporting tool among several.³
Brain-gut therapy, tailored to you
Fix the miscommunication between your back and brain
Overcome life's challenges
Take control of hot flashes and night sweats
Quit smoking in 3 weeks
Other tests your doctor may order alongside a Rome IV IBS diagnosis
Because several conditions produce symptoms that look like IBS – including celiac disease, inflammatory bowel disease (IBD), and thyroid problems – your doctor will use a small number of targeted tests alongside the Rome IV criteria to rule these out. Which tests you need depends on your symptoms, subtype, age, and whether any red flags are present.³
Blood tests commonly used in IBS assessment
Blood tests help identify conditions that can mimic IBS. Standard tests include a complete blood count (CBC) to check for anemia, C-reactive protein (CRP) to flag inflammation, and celiac disease antibodies (tissue transglutaminase IgA with total IgA) – especially for people with IBS-D or IBS-M.³
Stool tests: what they check for and why
Stool tests help distinguish IBS from inflammatory and infectious causes of gut symptoms. Fecal calprotectin or lactoferrin checks for gut inflammation (a marker of IBD), and a stool sample may be tested for infection if recent travel, antibiotic use, or food exposure makes that relevant.³
When a colonoscopy is (and isn't) needed for IBS
Colonoscopy is not routinely recommended for people under 45 without red flag symptoms. It's typically advised if you are 45 or older, have a family history of colorectal cancer or IBD, or have symptoms like rectal bleeding or unexplained weight loss.³
Hydrogen breath tests: checking for SIBO and food intolerances
Hydrogen breath tests aren't part of a standard IBS workup – they're used only when small intestinal bacterial overgrowth (SIBO), lactose intolerance, or fructose intolerance is specifically suspected based on your symptom pattern.⁵
Red flag symptoms that point to a condition other than IBS
Certain symptoms fall outside the typical IBS pattern and prompt your doctor to investigate further before confirming a diagnosis. These are known as red flags or alarm features – and recognizing them matters because they can point to conditions like inflammatory bowel disease (IBD), celiac disease, or colorectal cancer that need different treatment.³
Red flags include:
- Rectal bleeding or blood in your stool
- Unexplained weight loss
- New symptoms starting after age 50
- Symptoms that wake you from sleep at night
- Persistent fever
- Anemia or other abnormal blood results
- A family history of colorectal cancer, celiac disease, or IBD³
Having one of these features doesn't mean you have a serious condition – but it does mean your doctor will run additional tests before landing on an IBS diagnosis. If any of these apply to you, flag them clearly at your appointment so your doctor can investigate appropriately from the start.
How to prepare for your IBS diagnosis appointment
Coming into your appointment with clear, specific information about your symptoms is the single best thing you can do to speed up diagnosis. The Rome IV criteria rely on pattern recognition – so the more clearly you can describe your pattern, the faster your doctor can apply them.
What to bring to your appointment:
- A symptom diary covering at least two to four weeks, noting pain, bowel movements, and stool appearance (the Bristol Stool Chart is the standard tool)
- Known or suspected triggers – specific foods, stress, menstrual cycle changes, or time of day
- Family history of digestive conditions including IBD, celiac disease, or colorectal cancer
- A list of current medications, supplements, and any recent antibiotic use
- Any red flag symptoms (rectal bleeding, unexplained weight loss, night-time symptoms)
"Our IBS patients typically have suffered from five to seven years before they have seen me or somebody else and somebody has even diagnosed them with IBS." – Dr. Jeffrey Nathanson, Gastroenterologist, Comprehensive Gastrointestinal Health
That delay is exactly what a prepared appointment helps you avoid. Walking in with a clear symptom history – not just "my stomach's been bad" – gives your doctor what they need to confirm IBS in one visit instead of three.
Questions to ask your doctor at your IBS appointment
A short, specific list of questions keeps the appointment focused and makes sure nothing important gets missed:
- Do my symptoms meet the Rome IV criteria for IBS?
- Which IBS subtype do I have, and how does that affect my treatment options?
- Are there any tests you'd recommend to rule out other conditions?
- What first-line treatments do you suggest – including dietary, medical, and gut-brain therapy options?
- Should I be referred to a gastroenterologist, or can this be managed in primary care?
What happens after I’m diagnosed with IBS?
Once IBS is confirmed, the focus shifts from working out what's wrong to actively managing it – and the research is clear that the most effective approach combines strategies that target both your day-to-day symptoms and the underlying gut-brain mechanism driving them.³
IBS is classified as a gut-brain disorder, meaning your symptoms are maintained by visceral hypersensitivity and altered signalling between your gut and nervous system. Diet and medication can help manage triggers and immediate symptoms, but they don't directly address the neural amplification that keeps symptoms coming back. This is why major clinical guidelines recommend gut-brain therapy as first-line care, alongside diet and medication.³
Gut-brain therapy as a first-line option for IBS
Gut-directed hypnotherapy is one of the most well-researched forms of gut-brain therapy for IBS. It's designed to calm the overactive gut-brain signalling that drives symptoms like pain, bloating, and urgency – working on the underlying mechanism rather than the triggers.
Nerva is a 6-week gut-brain therapy program that delivers gut-directed hypnotherapy, cognitive-behavioral education, breathing techniques, and symptom tracking in 15–20 minutes per day at home. In the Nerva randomized controlled trial, 81% of participants achieved a clinically significant improvement on the IBS Symptom Severity Scale (IBS-SSS), and 71% had a clinically significant reduction in abdominal pain.⁶ Nerva helps manage IBS symptoms alongside dietary and medical care, and can be introduced early in your treatment plan rather than saved as a last resort.
Why early action matters after an IBS diagnosis
Starting treatment promptly after diagnosis – rather than waiting to see if symptoms resolve on their own – is consistently linked to better outcomes. Acting on multiple fronts at once (diet, medication, and gut-brain therapy) tends to produce stronger symptom control than relying on any single strategy, because each one targets a different layer of what's driving your symptoms.³
Frequently asked questions
How long does it take to get diagnosed with IBS?
IBS diagnosis can happen in a single appointment when your symptoms clearly meet the Rome IV criteria and no red flags are present. In practice, more than a quarter of people wait over five years from their first symptoms to a diagnosis – usually because the positive diagnostic approach isn't well known among patients or some clinicians.²
Can IBS be diagnosed by a blood test?
Blood tests cannot confirm IBS on their own, but they play an important supporting role – particularly for screening out celiac disease, inflammation, and anemia. Newer biomarker tests like IBS-Smart can support an IBS-D or IBS-M diagnosis but aren't recommended as a standalone diagnostic tool by major guidelines.⁴
Can you self-diagnose IBS?
Self-diagnosis isn't recommended because several conditions – including celiac disease, inflammatory bowel disease, and microscopic colitis – produce symptoms that closely mimic IBS and require very different treatment. Matching your symptoms against the Rome IV criteria is a useful starting point for a conversation with your doctor, not a substitute for formal diagnosis.³
Can IBS be diagnosed in children and teenagers?
IBS is diagnosed in children and adolescents using modified Rome IV criteria that account for age-appropriate symptom reporting. Pediatric IBS diagnosis typically involves a pediatric gastroenterologist, and gut-directed hypnotherapy is a first-line recommendation for functional abdominal pain in this age group.
Can IBS develop suddenly after a stomach infection?
IBS can develop suddenly after a gastrointestinal infection – this is called post-infectious IBS and accounts for a significant portion of new diagnoses. The mechanism involves lasting changes to gut-brain signalling that persist even after the original infection has resolved.
Do I need a referral to a gastroenterologist to get diagnosed with IBS?
A primary care doctor can diagnose IBS in most cases using the Rome IV criteria and basic tests. Referral to a gastroenterologist is usually reserved for people with red flag symptoms, atypical presentations, or those who haven't responded to first-line treatment.³
.jpeg)

.jpeg)






