Irritable bowel syndrome (IBS) comes in several distinct subtypes – IBS with constipation (IBS-C), IBS with diarrhea (IBS-D), IBS with mixed bowel habits (IBS-M), and unclassified IBS (IBS-U) – each with its own symptom pattern and management needs. Understanding which type you have is the first step toward finding the right treatment, diet, and gut-brain support for lasting relief.
What is IBS?
IBS is a gut-brain disorder affecting roughly one in ten people worldwide. At its core, it reflects a miscommunication between the brain and the gut – one that influences how food moves through the intestines, how the gut senses pain, and how it reacts to stress. When that connection becomes overly sensitive or out of sync, symptoms like bloating, cramping, and irregular bowel movements follow.
The most common symptoms of IBS include abdominal pain or cramps, bloating and gas, mucus in stools, and changes in bowel habits such as constipation, diarrhea, or both.
Understanding IBS subtypes
IBS is classified into subtypes based on the consistency and frequency of bowel movements. Identifying your IBS subtype can help guide more targeted management approaches.
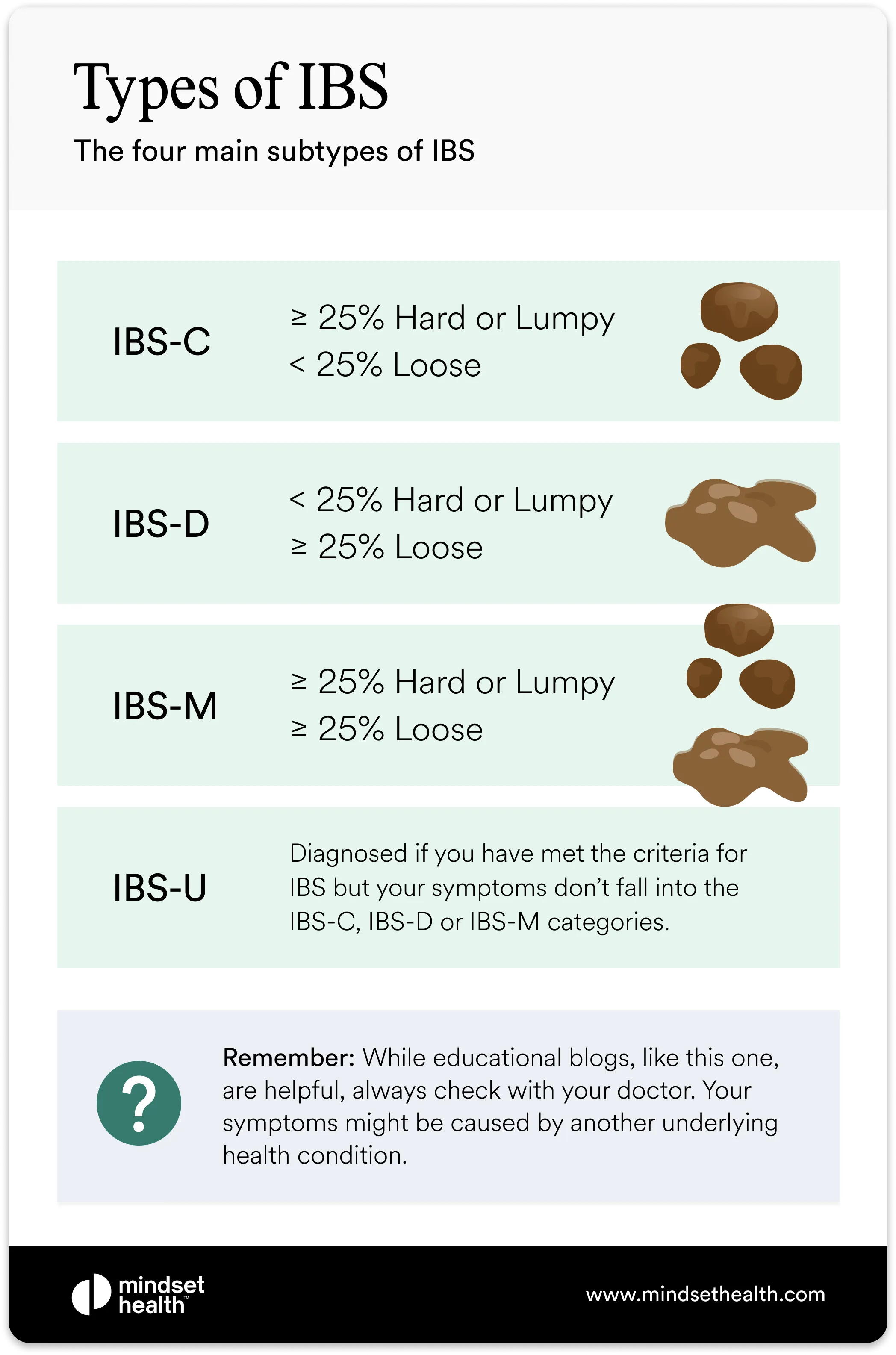
There are four main types: IBS-C, IBS-D, IBS-M, and IBS-U. Some people move between subtypes over time as their symptoms change.
In addition, some people may experience variations such as post-infectious IBS (PI-IBS) or post-diverticulitis IBS (PD-IBS), which occur following illness or inflammation in the digestive tract.
IBS with constipation (IBS-C)
IBS-C, or constipation-predominant IBS, is characterized by infrequent bowel movements and harder stools. For diagnosis, at least 25% of stools must be hard or lumpy, and fewer than 25% loose or watery.
Common symptoms of IBS-C include:
• Infrequent bowel movements
• Hard, lumpy stools
• Straining during bowel movements
• A sensation of blockage or incomplete emptying
People with IBS-C may also experience bloating, abdominal pain, and discomfort due to slower transit time through the colon. Treatment often focuses on dietary fiber balance, hydration, and techniques that regulate the brain-gut axis.
IBS with diarrhea (IBS-D)
IBS-D, or diarrhea-predominant IBS, is the most common subtype. It’s defined by more than 25% of stools being loose or watery and fewer than 25% being hard or lumpy.
Common symptoms of IBS-D include:
• Frequent bowel movements
• Loose or watery stools
• Urgent need to use the bathroom
• Cramping or discomfort relieved by bowel movements
Because IBS-D symptoms can be unpredictable, many people experience anxiety related to eating out, social situations, or travel. Management often includes calming the brain-gut connection, adjusting diet (such as following a low FODMAP plan), and practicing relaxation or mindfulness techniques.
IBS with mixed bowel habits (IBS-M)
IBS-M, also called mixed-type IBS or alternating IBS, involves both constipation and diarrhea. People with IBS-M experience inconsistent bowel habits, where stool consistency and frequency can vary daily or weekly.
For an IBS-M diagnosis, at least 25% of stools must be hard or lumpy and at least 25% loose or watery.
Common symptoms of IBS-M include:
• Alternating constipation and diarrhea
• Fluctuating stool consistency
• Abdominal pain and bloating that change with bowel habits
Because IBS-M combines features of both IBS-C and IBS-D, managing it requires flexibility and ongoing monitoring of triggers. A combination of dietary strategies, gut-focused therapies, and stress reduction techniques can help stabilize symptoms.
IBS unclassified (IBS-U)
IBS-U, or unclassified IBS, is diagnosed when symptoms meet the general criteria for IBS but don’t clearly fit into the constipation-, diarrhea-, or mixed-dominant categories.
Common symptoms of IBS-U include:
• Variable stool consistency
• Unpredictable bowel habits
• Abdominal discomfort or bloating
IBS-U often presents as a milder or shifting version of the other subtypes, though it can still significantly affect quality of life. Because it doesn’t follow a clear pattern, treatment focuses on identifying triggers, maintaining a consistent diet, and managing stress through brain-gut therapies.
Post-infectious IBS
Beyond the four main subtypes of irritable bowel syndrome (IBS), researchers also recognize additional classifications that develop after other digestive conditions. One of the most common is post-infectious IBS, which occurs when IBS symptoms begin after a gastrointestinal infection such as gastroenteritis.
After an infection, lingering inflammation, changes in gut bacteria, and increased intestinal permeability can disrupt the brain-gut connection, making the digestive system more sensitive and reactive. This altered environment can trigger long-term IBS symptoms even after the original infection has resolved.
Common symptoms of post-infectious IBS include:
• Abdominal pain or cramping
• Diarrhea or loose stools
• Nausea or vomiting
Studies suggest that up to one-third of people who experience a severe gastrointestinal infection go on to develop IBS symptoms, though about half of those may recover within six years. In some cases, treating residual inflammation and restoring gut flora balance can help ease ongoing symptoms.
Post-diverticulitis IBS
Post-diverticulitis IBS (PD-IBS) can develop after a person has recovered from diverticulitis, an inflammatory condition affecting small pouches (diverticula) that form in the lining of the intestine. When these pouches become infected or inflamed, they can cause abdominal pain, changes in bowel habits, and bloating.
Even after the infection clears, the intestines may remain hypersensitive, leading to IBS-like symptoms such as pain, urgency, and irregular bowel movements. People who have had diverticulitis are thought to be at higher risk of developing IBS, with symptoms that may fluctuate in intensity or duration.
Common features of post-diverticulitis IBS include:
• Ongoing abdominal pain or tenderness
• Changes in stool consistency
• Bloating and discomfort after meals
Management typically focuses on supporting the healing process, reducing inflammation, and regulating bowel function through dietary and behavioral interventions.
Managing IBS symptoms
Regardless of subtype, IBS can vary widely from person to person, which means management needs to be individualized. Both over-the-counter and prescription medications can relieve symptoms of IBS-C or IBS-D, but because treatments are subtype-specific, not every therapy works for everyone.
If medication isn’t effective or you prefer a non-pharmacological approach, other proven options are available. These include:
• Gut-directed hypnotherapy – a mind–body therapy that helps calm the nervous system and reduce symptom sensitivity.
• The low FODMAP diet – an evidence-based eating plan that limits fermentable carbohydrates known to trigger IBS symptoms.
A comprehensive approach that addresses diet, stress regulation, and the brain-gut connection tends to provide the best long-term relief for IBS across all subtypes.
Medications for IBS-C
Treatment for constipation-predominant IBS (IBS-C) focuses on improving stool consistency, reducing abdominal pain, and increasing the movement of food through the intestines. These medications target gut motility and fluid balance to relieve constipation and discomfort.
Common medications for IBS-C include:
• Lubiprostone (Amitiza) – Increases fluid secretion in the small intestine to enhance motility and make stools easier to pass. It’s typically prescribed when lifestyle and dietary changes haven’t provided relief.
• Linaclotide (Linzess) – Stimulates fluid secretion and accelerates bowel movement transit through the digestive tract. While effective for constipation, it can sometimes cause diarrhea as a side effect.
• Selective serotonin reuptake inhibitors (SSRIs) – Antidepressants such as fluoxetine (Prozac) and paroxetine (Paxil) can help reduce abdominal pain and support bowel regularity by improving communication along the brain-gut axis.
• Over-the-counter laxatives – Products such as magnesium hydroxide or polyethylene glycol (Miralax) can help improve stool frequency and softness, though they are generally recommended for short-term use under medical guidance.
Medications for IBS-D
For diarrhea-predominant IBS (IBS-D), medications are designed to slow intestinal transit, reduce pain, and restore balance to the digestive process. Because IBS-D can involve hypersensitivity and overactive motility, these treatments work to calm the gut and stabilize bowel function.
Common medications for IBS-D include:
• Alosetron (Lotronex) – Helps relax the large intestine, slow stool movement, and reduce motility. It’s approved only for women with severe IBS-D who haven’t responded to other treatments and is not prescribed for men.
• Tricyclic antidepressants (TCAs) – Low doses of medications such as imipramine (Tofranil) or desipramine (Norpramin) can help reduce abdominal pain and control diarrhea by modulating nerve signals between the brain and gut. Potential side effects include dry mouth, drowsiness, and blurred vision.
• Rifaximin (Xifaxan) – A gut-targeted antibiotic that may reduce bacterial overgrowth and improve diarrhea symptoms in IBS-D. It’s typically prescribed for short treatment courses and may be repeated if symptoms return.
These medications can be effective when tailored to the specific IBS subtype and used as part of a broader management plan that includes diet, lifestyle, and stress regulation to support long-term brain-gut balance.
Brain-gut therapy, tailored to you
Fix the miscommunication between your back and brain
Overcome life's challenges
Take control of hot flashes and night sweats
Quit smoking in 3 weeks
Psychological management of IBS subtypes
Psychological therapies are an important part of treating all IBS subtypes. These approaches don’t suggest that IBS is “all in your head.” Instead, they work by calming the nervous system and improving communication along the gut-brain connection, helping reduce symptom intensity and frequency across different IBS presentations.
Gut-directed hypnotherapy for IBS: restoring calm and gut balance
Gut-directed hypnotherapy uses guided relaxation and imagery to retrain how the brain and gut communicate. By lowering gut sensitivity and easing stress-driven motility changes, hypnotherapy has been shown to reduce key symptoms such as abdominal pain, bloating, and irregular bowel habits.
Research consistently shows that gut-directed hypnotherapy is one of the most effective psychological treatments for IBS, improving symptoms in around 70% of patients, regardless of subtype.
Cognitive behavioral therapy (CBT) for IBS: retraining thought and symptom response
Cognitive behavioral therapy (CBT) helps people identify and change unhelpful thought patterns that can worsen IBS symptoms. For those living with IBS-C, IBS-D, or IBS-M, CBT reduces symptom-related anxiety, normalizes bowel habits, and supports a more balanced stress response.
Studies show that CBT is highly effective in improving quality of life and reducing abdominal discomfort by helping patients reframe their relationship with their symptoms and stress triggers.
Watch a GI psychologist explain the differences between GDH and CBT.
Yoga for IBS: movement-based stress reduction
Yoga combines breathing, stretching, and relaxation to support both physical and emotional regulation. For people with IBS, yoga helps regulate autonomic function, reduce cortisol levels, and ease tension that can worsen constipation or diarrhea.
Regular yoga practice improves the gut-brain connection and has been shown to relieve bloating, pain, and stress across multiple IBS subtypes. Even gentle, restorative poses can calm the digestive system when practiced consistently.
Discover the best yoga poses to relieve IBS pain.
Mindfulness meditation for IBS: calming the symptom–stress cycle
Mindfulness meditation encourages awareness of the present moment and reduces emotional reactivity to gut sensations. This helps interrupt the symptom–stress–symptom cycle that often fuels IBS flare-ups.
Clinical research shows mindfulness-based approaches significantly lower stress, ease abdominal discomfort, and help patients respond to symptoms with less anxiety and tension. Short, daily mindfulness sessions can meaningfully reduce symptom severity for all IBS subtypes.
Best dietary treatments for IBS subtypes
Diet is one of the most powerful tools for managing irritable bowel syndrome (IBS) – but not all IBS subtypes respond the same way. Because IBS is a Disorder of Gut–Brain Interaction (DGBI), food choices can directly affect gut motility, sensitivity, and inflammation. Adapting dietary strategies to your IBS subtype can help regulate bowel habits and reduce flare-ups.
Best diet for IBS-C (constipation-predominant)
For people with IBS-C, supporting regular bowel movements is the main goal. Increasing soluble fiber intake – found in oats, psyllium husk, chia seeds, and flaxseed – can help soften stools and improve consistency. Staying hydrated and maintaining consistent meal timing are also key for stimulating motility.
Many patients with IBS-C benefit from limiting insoluble fiber (like bran) and high-fat foods that can slow digestion. Gentle movement, regular meals, and brain-gut calming practices such as yoga or hypnotherapy further support digestive balance.
Best diet for IBS-D (diarrhea-predominant)
For IBS-D, the aim is to calm rapid motility and reduce bowel urgency. Avoiding trigger foods such as caffeine, alcohol, and fried or spicy meals can help. Adding soluble fiber sources like oats or bananas can absorb excess water in the gut and improve stool formation.
It’s also helpful to avoid artificial sweeteners (like sorbitol and mannitol) and to limit lactose if you notice sensitivity. Many people with IBS-D see improvement when combining dietary adjustments with relaxation or mindfulness-based stress management.
Best diet for IBS-M (mixed bowel habits)
IBS-M (also known as alternating-type IBS) involves both constipation and diarrhea, so dietary balance is key. A moderate-fiber diet with stable hydration helps minimize extremes. Because IBS-M symptoms shift, keeping a food and symptom diary can identify patterns and prevent over-restriction.
The low-FODMAP diet, when tailored by a dietitian, is particularly effective for IBS-M, as it helps reduce bloating, gas, and unpredictable bowel changes.
Best diet for IBS-U (unclassified type)
People with IBS-U may not fit neatly into the main subtypes but still experience bloating, discomfort, or inconsistent bowel habits. A gentle approach focused on balanced, whole foods and regular meal timing works best. Limiting processed foods, reducing caffeine, and supporting hydration can ease symptoms and improve gut stability.
The low-FODMAP diet for IBS symptom relief
The low-FODMAP diet, developed by Monash University, is the most researched dietary approach for all IBS subtypes. FODMAPs (fermentable oligosaccharides, disaccharides, monosaccharides, and polyols) are short-chain carbohydrates found in foods like wheat, onions, garlic, apples, and milk.
These carbohydrates can be poorly absorbed in the small intestine, leading to gas, bloating, and pain as they ferment in the gut. The low-FODMAP diet involves three steps:
- Elimination – temporarily removing high-FODMAP foods.
- Reintroduction – testing one FODMAP group at a time to identify triggers.
- Personalization – building a long-term, balanced diet based on tolerance.
Around 70% of people with IBS experience significant improvement when following a low-FODMAP plan under dietitian supervision.
Final thoughts on diet and IBS management
Each IBS subtype interacts differently with food, but the underlying mechanism – a sensitive brain-gut connection – is shared. Understanding how your body responds to certain foods is one of the most effective ways to take control of your symptoms.
Combining dietary modification with medical and psychological support can help regulate digestion, reduce pain, and restore confidence in daily eating. With professional guidance and consistent self-awareness, most people can achieve long-term relief and improved gut function.
Frequently asked questions
What are the subtypes of IBS?
IBS has four subtypes based on bowel habit pattern: IBS-C (constipation), IBS-D (diarrhea), IBS-M (mixed), and IBS-U (unclassified). Each subtype is defined by the proportion of stools that are hard versus loose, using the Rome IV diagnostic criteria.
Can IBS go away permanently?
IBS is a long-term gut-brain disorder, but symptoms can improve significantly and many people experience extended periods of remission. Gut-brain therapy programs like Nerva have been shown in clinical trials to produce lasting symptom relief well beyond the active treatment period.
Can your IBS subtype change over time?
IBS subtypes are not fixed – it is common to move between IBS-C, IBS-D, and IBS-M as symptoms shift over time. This is why treatment tends to focus on the underlying gut-brain mechanism rather than a single symptom pattern.
What is the most common type of IBS?
IBS-D (diarrhea-predominant) is the most commonly diagnosed subtype, affecting around 46% of people with IBS. IBS-C and IBS-M are also widely prevalent, with many people unaware their symptoms fit a specific subtype until formally diagnosed.
Does IBS subtype affect which treatment works?
IBS subtype guides some treatment choices, particularly for diet and medication. Gut-brain therapy programs like Nerva work across all subtypes because they target the nervous system hypersensitivity driving IBS regardless of bowel habit pattern.
.jpeg)